



Who we are
The Chronic Care Center is a medico-social institution, specialized in the treatment and follow-up of childhood chronic diseases: Thalassemia and Type I Diabetes.
Know The Signs
My baby is very pale and has no energy to play. He does not seem to be growing well even though he eats well. I am worried How can I know if he has thalassemia?
How can I know if he has thalassemia?
You consult your child's pediatrician. He will ask for a complete blood count to rule out anemia
What is Thalassemia?
Thalassemia is a genetically inherited blood disease, found in many countries around the world, particularly in people of Mediterranean, Middle-Eastern and Asian origin. The two main types of Thalassemia are: Thalassemia Trait and Thalassemia Major. There is another less severe form of the disease called Thalassemia Intermedia. In this case, patients need less frequent blood transfusions to improve their quality of life, but not in order to survive.
When a person inherits one defective gene, he is said to have Thalassemia trait or he is a carrier. This is not a disease. It is a transmissible recessive trait. That is why prevention at this level is so important.
Thalassemia Major is an inherited genetic disease that is passed from parents to children through the genes. It is not infectious and cannot be passed on from one individual to another by personal or any other contact, through blood transfusion, food or air.
It is a serious anemia that usually starts at 3 months to 2 years of age. Treatment of Thalassemia Major requires frequent blood transfusions and continuous chelation therapy to keep the iron level normal in the blood and other vital organs.
Thalassemia Carriers or Trait are individuals who have inherited a normal haemoglobin gene from one parent and the defective gene from the other parent.
They have no physical or mental symptoms and do not require a special diet or medical treatment. The condition cannot become a serious disease over time - indeed, most carriers will be unaware that they carry the trait unless specifically tested.
How is it inherited?
Thalassemia Major can be inherited when both parents are carriers of Thalassemia.
There are three possible outcomes at every pregnancy:
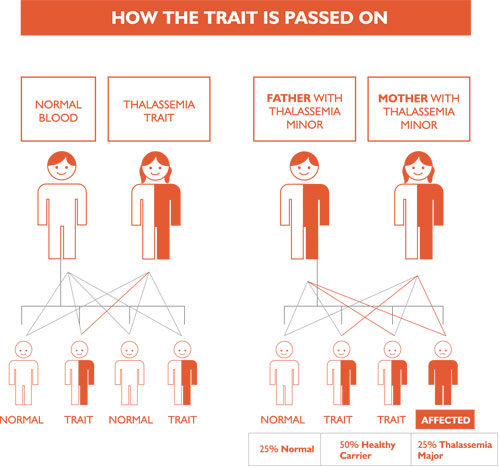
The risk of having Thalassemia child:
If both parents are carriers, the risk of having a Thalassemia child is 25 % with every pregnancy; therefore, each pregnancy carries a 1 in 4 risk of delivering a patient with Thalassemia.
What is the Carrier rate and the expected number of Newborns affected with the disease?
Worldwide:
- An estimated 7% of the global population is a carrier of an abnormal, or pathological, hemoglobin gene.
- Some 300,000 - 500,000 children with a severe hemoglobin disorder are born each year, of whom 30% have Thalassaemia.
In Lebanon:
- The carrier rate is estimated to be 2-3 %.
- The Chronic Care Center, the only specialized institution for the treatment of Thalassemics in Lebanon carried a study in 2000 on 2701soldiers representing the Lebanese community and confirmed a 2.3 % carrier rate.
- The expected number of newborn Thalassemia patients according to WHO document in 1994 is 46 ß Thalassemia patients per year.
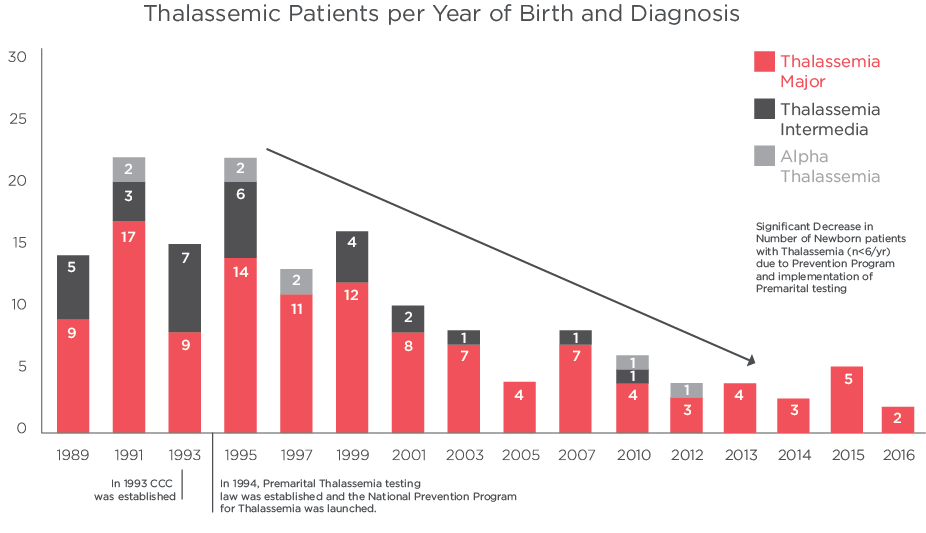
- Data from the Chronic Care Center, shows that the number of new Thalassemia patients born have decreased by 75 %, from more than 20 cases / year in 1994 to less than 5 in the last 6 years before 2017.
Why do we need to prevent Thalassemia?
- The disease is preventable.
- It is easily detectible by doing a blood test: Hemoglobin Pattern testing using High Performance Liquid Chromatography (HPLC) technique.
Carriers will have an HbA2> 3.5% (borderline levels 3.1-3.5% need further genetic testing for confirmation).
- It necessitates life time treatment and regular medical follow-up including frequent blood transfusions.
- The treatment of the disease is very costly (10,000-30,000$/year/patient).
- The financial, medical and psychological burden of this condition is very heavy on the patient, family and the society at large.
Prevention is an effective tool to reduce the number of birth of affected children and can ultimately lead to the eradication of the disease. It contributes to building healthier generations.
How to prevent Thalassemia?
Before marriage:
- Test yourself to know if you are a carrier of Thalassemia by performing hemoglobin testing by HPLC technique.
Perform the test in a reliable laboratory and consult a hematologist for the interpretation of the results. This test is available at the Chronic Care Center. - If you are about to get married take seriously the premarital testing.
- If you are carrier and your partner too, you should know the risks of having a thalassemic child and the options to prevent it.
For more information, you can consult a hematologist or contact the prevention unit at the Chronic Care Center.
After marriage
- If one partner is healthy and is not carrier, there is no risk of having a Thalassemic child.
However, if one parent is a carrier, children may be carriers like their parent. They should have their blood tested at some time before they have children of their own. - If both partners are Thalassemia carriers, there are several options but the decision differs due to cultural and religious beliefs.
-
- They can decide not to have a child or more.
- They can decide to do prenatal diagnosis (test the baby before birth) through geneting testing of fetus early in pregnancy by:
-
- Chorionic Villous Sampling (CVS), sampling of placental tissue at 10-12 weeks of gestation.
- Amniocentesis, by a small needle 30 ml of amniotic fluid is removed and tested for fetal defects at 16 weeks of gestation.

Genetic testing of blastomers, Preimplantation Genetic Diagnosis ( PGD) using IVF technique
Pre-implantation genetic diagnosis (PGD) for β-Thalassemia and/or Sickle Cell Anemia represents an alternative within prenatal diagnosis services, providing couples the chance to start a pregnancy with an unaffected fetus.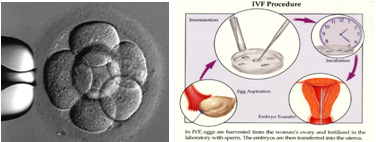
Patients aiming for PGD have to go through in vitro fertilization (IVF). Embryos obtained by in vitro fertilization (IVF) are tested for genetic disorders prior to their implantation in the uterus and before the pregnancy’s onset
All above tests are available in the laboratories of the Chronic Care Center
The Prevention Program at the Chronic Care Center:
This National program was launched in 1994 in collaboration with the Ministry of Social Affairs. It targets the general population, high risk groups and families of patients. It includes educational activities, screening and data analysis.
1. Education
- Awareness Campaigns at the national level to inform about the disease and to promote premarital test.
Around 8000 persons per year are attending these sessions (in villages, schools, universities, etc...)



- Training of trainers
The Center provides training for around 100 health professionals per year to promote awareness in their community all over the Lebanese regions. - Publication of educational material: books brochures posters
- Celebration of World Thalassemia Day, 8th of May every year.



2. Screening:
- The Chronic Care Center organizes campaigns for free screening (testing) to identify new carriers in the general population ( schools, universities) and high risk group: (brothers/sisters, cousins, family members of Thalassemics).


- The Genetics Laboratory provides counseling of identified carriers and prenatal tests:
- Genetic testing of CVS or amniotic fluid.
- Pre-implantation Genetic Diagnosis for Beta Thalassemia.
3. Surveillance:
- Updated registry of Carriers and patients at the Center and data analysis.
- Collaboration with policymakers at the Ministry of Public Health.
Lebanon a Success Story:
The prevention program along with the implementation of the Premarital Law by the Ministry of Public Health succeeded in decreasing the number of newborns with Thalassemia Major by more than 75% despite the legal and cultural limits.
Data showed that the average number of newborns before and after 1994 were: 20 cases / year for 8 years before 1994 and less than 5 cases / year for the last 6 years.
Graph 1
Graph 2
Diabetes Type1:
commonly occurs in childhood, rarely in adults.
commonly occurs in childhood, rarely in adults.
CAUSES
Genetic and environmental factors leading to changes in islet cells and destruction of ß cells, either directly or by triggering an autoimmune response.
TREATMENT
- The only treatment until now is insulin (injections-pump)
- Blood glucose self-monitoring.
- Diet.
- Exercise.
Acute complications:
Hypoglycemia: (BG < 60 mg/dl)
Causes:
- Not enough food
- Delayed or missed meals
- High dose of insulin
- Increased activity (exercise)
- Presence of renal failure
- Alcohol intake
- Change in injection site
Symptoms:
- Hunger
- Tremor
- Dizziness.
- Sweating.
Management:
- Give the conscious patient 15-20g of glucose or simple sugar and repeat after 15 min if necessary. Follow with long - acting carbohydrates (bread, plain biscuits, milk)
- If unconscious don’t give anything orally, call the doctor or diabetes educator.
Hypoglycemia: (BG < 180 mg/dl)
Causes:
- Untreated diabetes
- Too much food or imbalanced type of food
- Insufficient medication or incorrect dose
- Overuse of particular injection sites
- Poor injection technique
- Reduction of activity
- Infection / illness
- Increase of concurrent medication affecting glycemic control.
- Stress, life changes.
Symptoms:
- Polyuria
- Increased urination
- Polydipsia, extreme thirst
- Irritability.
- Visual changes...
- Weakness
- Weight loss
Actions to be taken:
- Adjustments may be required according to identified causes of the high blood sugar levels, regarding food, activity, medication, insulin.
- Test urine for the presence of ketones each time the b blood test is >240 – 300 mg/dl.
- If ketones are present call doctor or diabetes educator.
IMPORTANCE OF CONTINUOUS EDUCATION
Patient education has proven to be an essential mean in helping people with diabetes to accept their disease and deal with it; acquire scientific knowledge and skill to achieve autonomous self – management, resulting in a positive attitude for a good social integration.
EDUCATION OBJECTIVES
Social:
- Work on acceptance of the child’s situation.
- Help restore balance in the family home, working with all member of the family.
- Trusting the diabetic patient and avoiding over protection/li>
- Work on improving self-esteem
- Treating the diabetic child as an independent person, not different from his siblings or peers and capable to succeed in life.
- On the community level, work with patient’s surrounding (peers, schools, work environments), in order to promote social integration through acceptance.
Social objectives are achieved through:
- Regular follow-ups to provide individual and family support.
- Organizing recreational activities and summer camps, encouraging the exchange of personal experiences.
- Organizing educational sessions about diabetes, to promote awareness.
- Organizing regular parent committee meetings, to discuss problems encountered and support new cases.
Medical:
- Understand diabetes and its treatment.
- Acquire a good level of scientific knowledge and develop practical skills, concerning insulin treatment, blood glucose self-monitoring, as assets for the prevention of complications.
- Develop decision-making skills, in the matter of adjusting insulin doses, anticipation of scheduled events, such as special occasions or competitive sports, alcohol, smoking.
- Learn how to manage acute complications and reduce their risk (hypoglycemia, hyperglycemia, ketonuria).
- Reduce and prevent long term complications by trying to achieve a tight control of diabetes, and an HbA1c closest to normal (<7%).
- Encourage taking charge of diabetes management, promoting autonomous individuals, to ensure a satisfactory life style.
N.B: Education is given for diabetic patients and their significant others in the center during follow-up visits by using dynamic group and individual interviews.
Nutritional:
- Patient assessment
- Evaluating individual dietary habits, lifestyle and physical activity.
- Goal-setting, individualized dietary instruction and periodic evaluation and modification.
- Develop an individualized plan, which meets the nutritional needs of every child with diabetes, ensuring adequate and normal growth and development and limiting glycemic fluctuations by adopting a regular meal distribution pattern.
- Encourage an active lifestyle; regular activity enhances longterm weight maintenance and improves insulin sensitivity, glycemic control, aerobic fitness and selected risk factors.
- Learning how to make healthier food choices, and how to read nutritional labels of food products.
- Since carbohydrate consumption is a strong predictor of glycemic response, learning how to estimate carbohydrates is a good strategy to achieve glycemic control. Counting carbohydrates can be done using both the exchange system or the more advanced carbohydrate counting.
- Develop problem-solving skills: how to interpret blood glucose monitoring results and make adjustments.
- Follow-up visits evaluate the outcome of self- management, supplement nutritional information and problem-solving strategies and modify the diet plan as needed (growth needs, beginning of chronic complications such as nephropathy, other needs).
AWARENESS BUILDING
The C.C.C. multidisciplinary team is committed to community education concerning diabetes and tries to reach the Lebanese population by:
- Supervising students training in the center, all programs and levels included and assisting them to prepare their papers and studies.
- Participating in training diabetes educators
- Annual conference on the Diabetes International Day, November 14.
- Educational material:


WHAT IS THALASSEMIA?
Thalassemia is a genetically inherited blood disease found in many countries around the world, particularly in people of Mediterranean and Asian origin and to a lesser degree among Northern Europeans. The word Thalassemia comes from the Greek "Thalasso" meaning sea and "hemia" meaning blood that is anemia of the sea.
TYPE OF THALASSEMIA ?
There are two kinds of Thalassemia: Thalassemia Trait and Thalassemia Major.
Thalassemia trait is not a disease. People who have thalassemia trait (carriers) carry one thalassemic gene and are completely healthy and live a normal life. However, they can transmit their thalassemic gene to their children. If they get married to a person who carries a thalassemic gene, then their children are at risk of having the disease, thalassemia major. That's why all marriage partners must undergo testing for the carrier state before marriage and before deciding to have children. It is estimated that 3% of the Lebanese population carry the beta thalassemia gene.
Thalassemia trait is not a disease. People who have thalassemia trait (carriers) carry one thalassemic gene and are completely healthy and live a normal life. However, they can transmit their thalassemic gene to their children. If they get married to a person who carries a thalassemic gene, then their children are at risk of having the disease, thalassemia major. That's why all marriage partners must undergo testing for the carrier state before marriage and before deciding to have children. It is estimated that 3% of the Lebanese population carry the beta thalassemia gene.
Thalassemia Major is a serious inherited blood disorder. Children born with this disorder have severe anemia because they cannot make enough hemoglobin in their blood. They present at about 3 months to 2 years of age with pallor, lack of appetite, loss of activity and abdominal distension. If not treated, they die in the first few years of life from anemia and its complications. If treated, they live a close to a normal life.
OUR STRATEGIC PLAN AIMS AT
Increasing awareness and spreading knowledge, through:
- Development of a national education and awareness strategy.
- Design of a “national network of partners and volunteers”.
- Production and dissemination of education and awareness material.
- Building local capacities and skills.
- Launching of well-planned sensitization and awareness campaigns.
Undertaking national screening & other community-
based initiatives, though:
- Development and execution of a national screening strategy.
- Reinforcement of the basic underlying concepts.
- Encouraging an effective implementation of the obligatory pre-marital certificate.
- Determination and execution of warranted research studies based on a proper needs’ assessment.
- Encouraging the establishment of a national registry for thalassemia.
- Publication and dissemination of results and recommendations of conducted studies.
Conducting research and statistical studies, through:
AWARENESS BUILDING & IMPLEMENTATION OF THE PROGRAM:
Main activities, The prevention program focuses on:
- Information about the disease(refer to section about thalassemia).
- Importance of blood donation to support the need of thalassemic patients.
- The paramount importance of the premarital exam and specifically in preventing thalassemia; highlighting the necessity of performing Hemoglobin Electrophoresis.
- Awareness about premarital diagnosis for high risk pregnant women.
- Screening for thalassemia carriers, with a main focus on high risk groups.
- Family planning for parents of thalassemics.
- Counseling of thalassemia carrier couples before marriage.
- Organizing annual conference on the Thalassemia International Day, May 8.
Target groups: the Educational program targets different groups namely:
- Patients & parents.
- Extended families (cousins, uncles, 2nde degree relatives …).
- High risk groups.
- Students who visit the Center
- Students in universities, secondary and technical schools.
- Medical Community: students in the health care field, training at the Center, nurses in medical centers & dispensaries.
Educational material
Questions and Answers Online
If you have a specific question about Thalassemia, you
can write us now
If you have a specific question about Thalassemia, you
can write us now